Department of Repertory
Shree Vidyadhiraja Homoeopathic Medical College
About
Serious intellectual endeavor starts with passion and curiosity. The Department of Repertory is a place where faculty and students intensely discuss what they love—novels, poems, paintings, films, comics—along with theoretical, philosophical and logical questions related to the study of Homoeopathy and Repertory. As part of a course of intensive study, these conversations spark intellectual excitement while building toward at the end a passion to Homoeopathy. Through the wide variety of interactive approaches in classes, they cultivate the analytical capacities that will continue to serve them in their personal and professional lives long after graduation.
The mission of the Department of Repertory undergraduate curriculum is to provide students with a thorough grounding in Repertorial knowledge. The department encourages our students to integrate the concerns of other fields into their studies and therefore maintains close links with other departments along with other academic programs.
NEWSLETTER













































































REPERTORY COLOSSEUM
DECODING THE SOUL OF SOCIAL WORLD
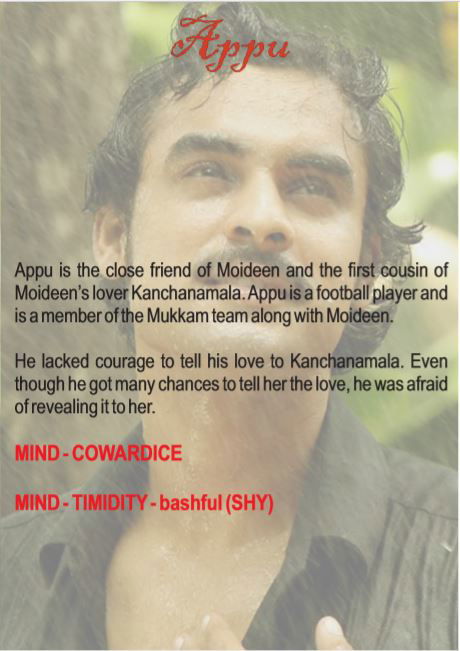
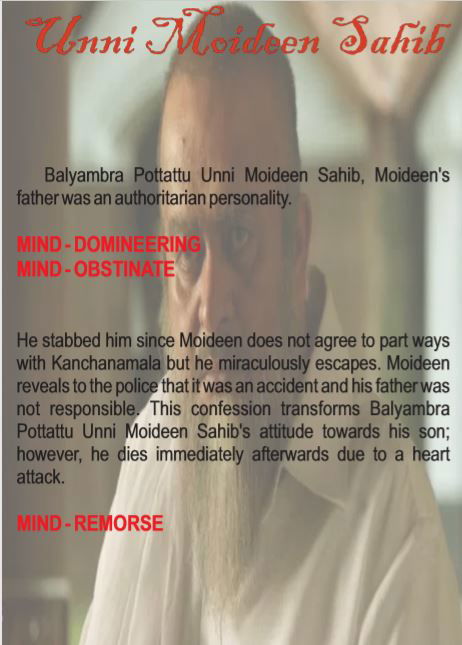
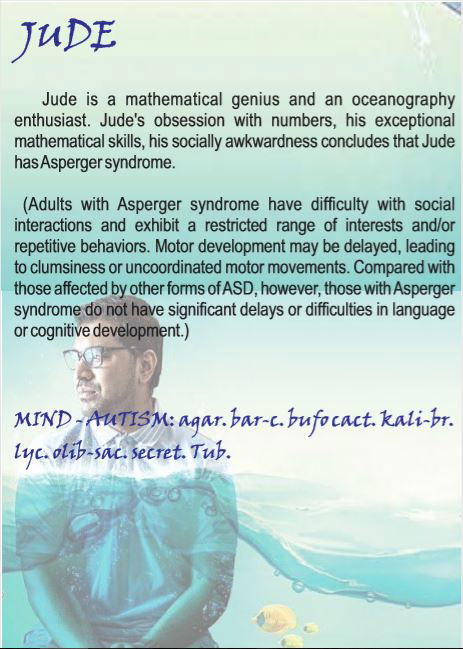
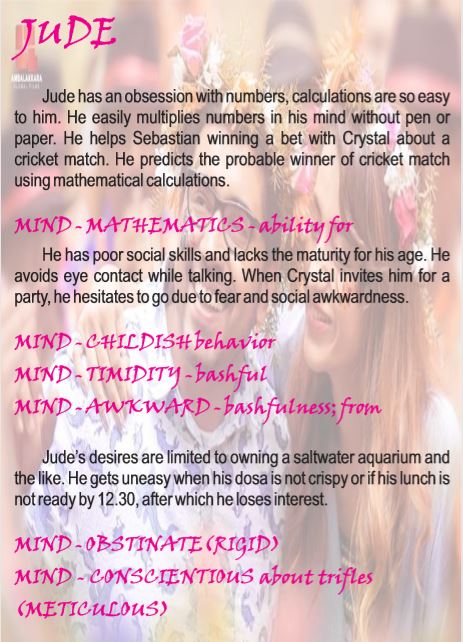
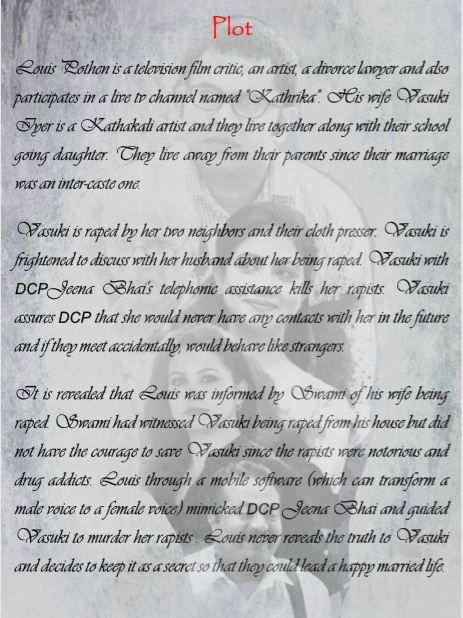
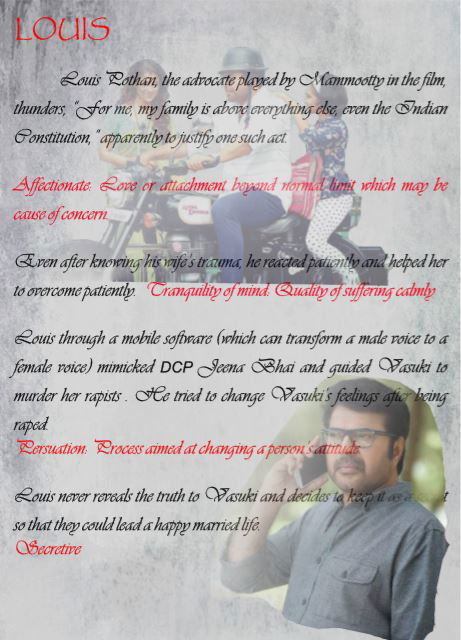
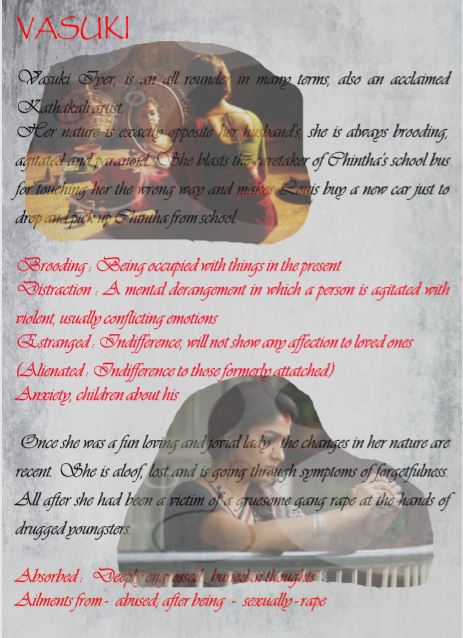
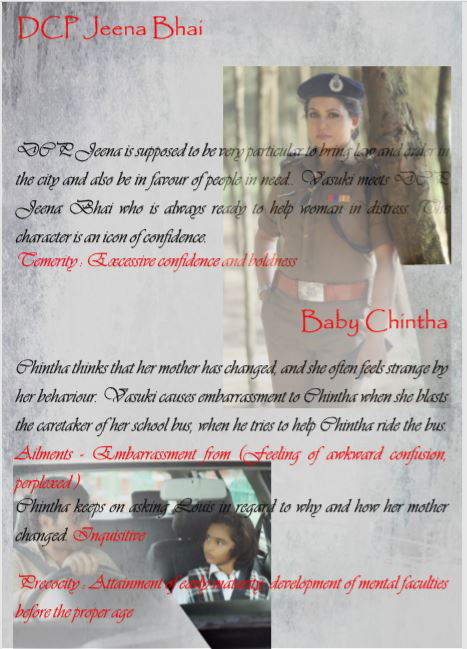
 " Selection of appropriate rubric(s) is a daunting challenge. As a Homoeopath, he needs a watchful eye to observe, to circumspect and to scrutinize. Context, situation and factual data gained through skillful interview coupled with the art of translating the patient’s language into the reportorial language help select the appropriate rubrics. Command over language has no alternative" .... Dr Ajit Kulkarni
" Selection of appropriate rubric(s) is a daunting challenge. As a Homoeopath, he needs a watchful eye to observe, to circumspect and to scrutinize. Context, situation and factual data gained through skillful interview coupled with the art of translating the patient’s language into the reportorial language help select the appropriate rubrics. Command over language has no alternative" .... Dr Ajit Kulkarni
REPERTORY SYLLABUS
REPERTORY SYLLABUS
IIIrd BHMS - THEORY
1. Repertory: Definition; Need; Scope & Limitations.
2. Classification of Repertories
3. Study of different Repertories (Kent, Boenninghausen, Boger-Boenninghausen): History Philosophical background Structure Concept of repertorization, Adaptability Scope Limitation(s)
4. Gradation of Symptoms by different authors.
5. Methods and techniques of repertorisation. Steps of repertorisation.
6. Terms & Language of repertories (Rubrics) Cross references in other Repertories and Materia Medica.
7. Conversion of symptoms into Rubrics and repertorisation using different repertories.
8. Repertory – its relation with Organon of Medicine and Materia Medica.
9. Case taking and related topics:
9.1. Case taking.
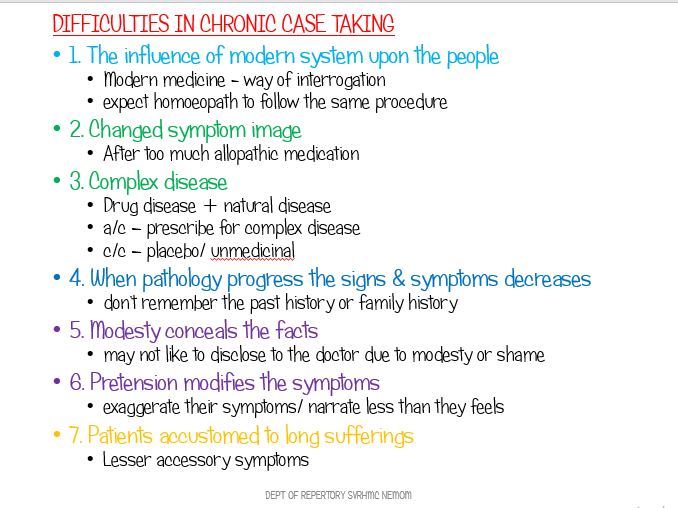
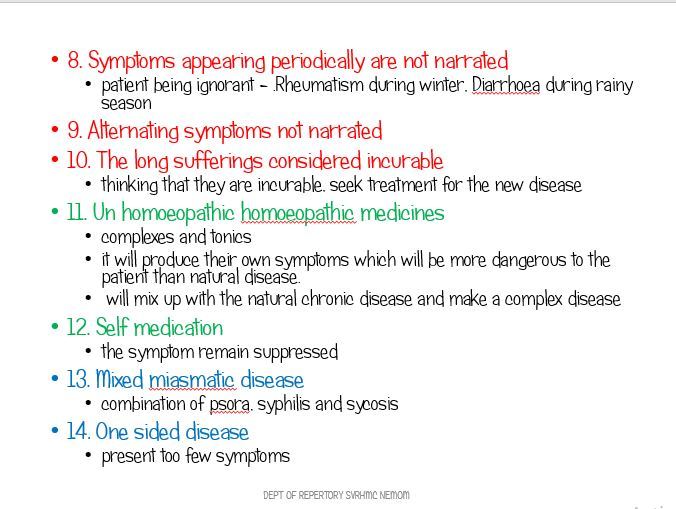
9.2. Difficulties of Case taking, particularly in a Chronic case.
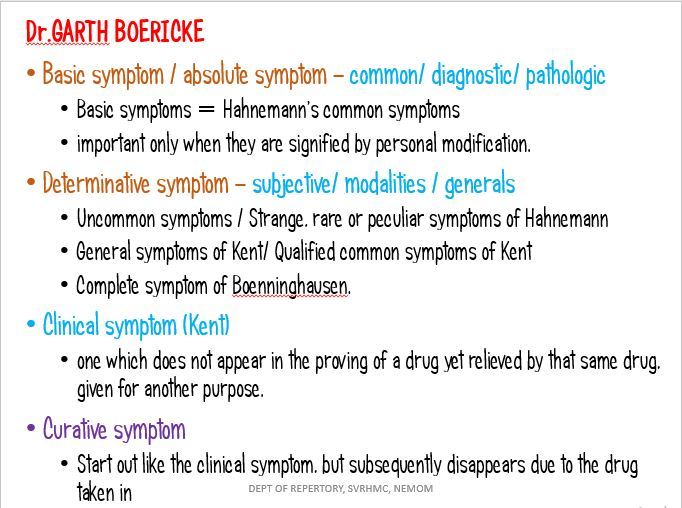
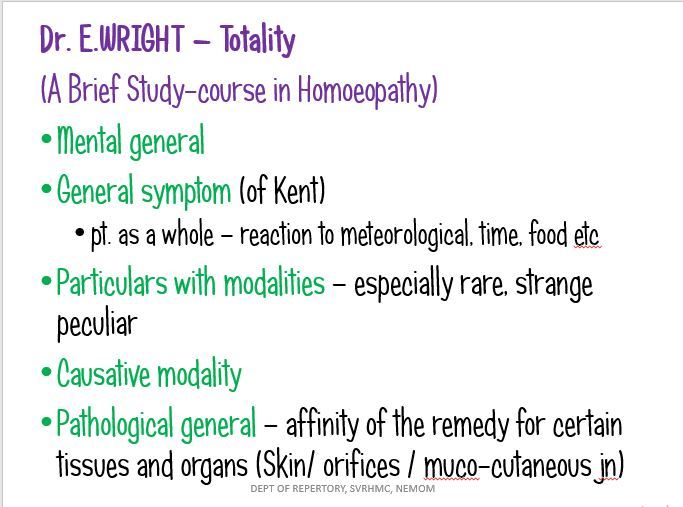
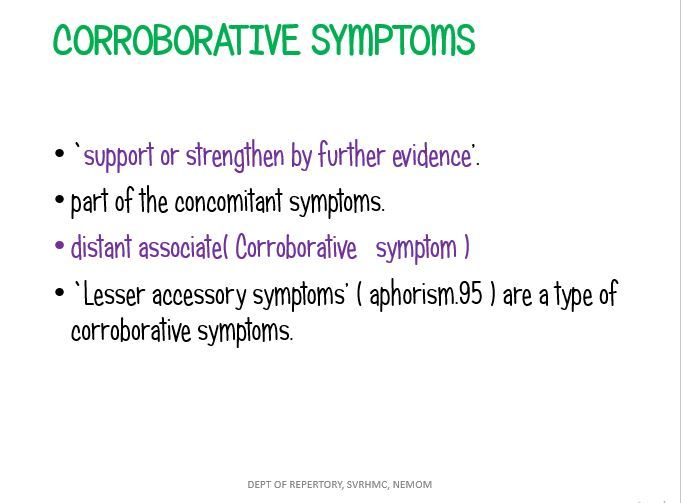
9.3. Types of symptoms, their understanding and importance.
9.4. Importance of Pathology in disease diagnosis & individualization in relation to study of Repertory.
10. Case Processing – -Analysis & Evaluation of symptoms -Miasmatic assessment -Totality of Symptoms/Conceptual image of the patient -Reportorial totality -Selection of rubrics -Repertorial technique and results -Repertorial analysis
Practical/Clinical Work Record of 05 cases each of Surgery, Gynaecology and Obstetrics worked out by using Kent‟s Repertory. Rubrics hunting from Kent‟s & Boenninghausen‟s Repertories.
IVth BHMS
1. Comparative study of different repertories (like Kent‟s Repertory, Boninghausen‟s Therapeutic Pocket Book and Boger-Boninghausen‟s Charactetristic Repertories, A Synoptic Key to Materia Medica).
2. Card Repertories – History, Types & Use.
3. Concordance Repertories (Gentry & Knerr)
4. Clinical Repertories (William Boericke etc.)
5. An introduction to modern Repertories- (Synthetic, Synthesis & Complete Repertory & Murphy‟s Repertory) 6. Regional Repertories
7. Role of Computers in Repertorisation and different softwares.
PRACTICAL Record of:
1. 10 acute & 10 Chronic cases (each of Medicine, Surgery and Obstetrics & Gynaecology) using Kent‟s Repertory
2. 05 cases (pertaining to Medicine) using Boenninghausen‟s Therapeutics Pocket Book.
3. 05 cases (pertaining to Medicine) using Boger-Boenninghausen‟s Characteristics Repertory.
4. 05 cases to be cross checked on Repertories using Homoeopathic softwares.
NEW SCHEME
Repertory
OBJECTIVES
1. Make the students competent enough to take cases in different clinical conditions and situations
2. Successful application of knowledge of repertory in day today clinical practice including management of acute diseases
3. Creating awareness about information and communication technology (ICT) in homoeopathy through medical apps and softwares
INSTRUCTIONS:
I (a) Repertorisationis not the end but the means to arrive at the similimum with the help of material medica based on sound knowledge of homoeopathic philosophy;
(b) Homoeopathic materiamedica is an encyclopedia of symptoms. No mind can memorize all the symptoms of all the drugs with their gradations;
(c) The repertory is an index and catalogue of the symptoms of the materiamedica nearly arranged in a practical or clinical form with the relative gradation of drugs, which facilitates quick selection of indicated remedy and it may be difficult to practise homoeopathy without the aid of repertories.
II (a) each repertory has been compiled on distinct philosophical base, which determines the structure;
(b) In order to explore and derive full advantage of each repertory, it is important to grasp thoroughly its conceptual base and construction and this will help students to learn scope, limitations and adaptability of each repertory.
Third BHMS
A. Theory:
1. Case taking and related topics:
(a) Case taking
(b) Difficulties of case taking, particularly in a chronic case.
(c) Types of symptoms, their understanding and importance
(d) Importance of pathology in disease diagnosis and individualisation in relation to study of repertory. Correlation of other clinical and nonclinical subjects in case taking and repertorisation. Repertory- its relation with organon of medicine and materiamedica
(e) Case taking in different clinical conditions and situations
(f) Reportorial approach in case taking
(g) Standardised case record. Different methods of record keeping
(h) Application of knowledge of repertory in acute diseases
2. Case processing
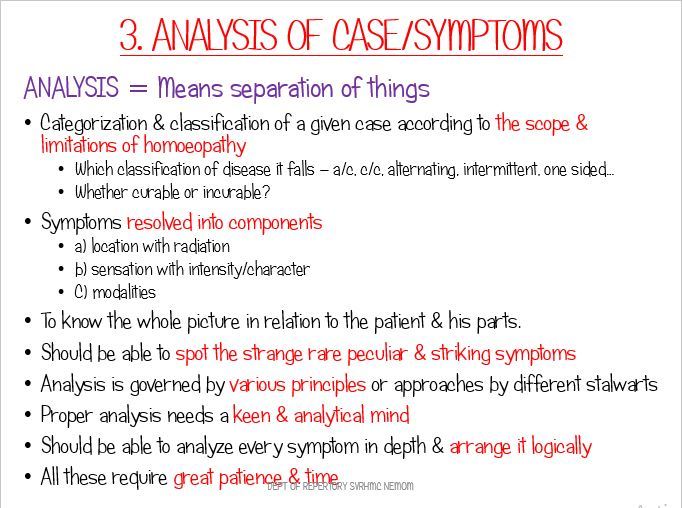
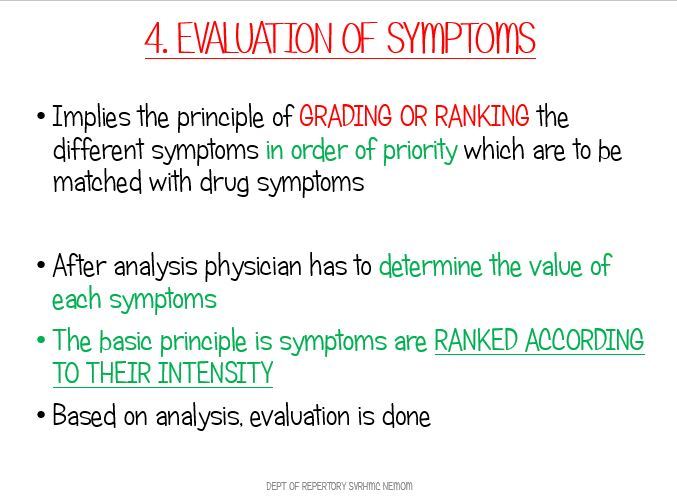
(a) Analysis and evaluation of symptoms
(b) Miasmatic assessment
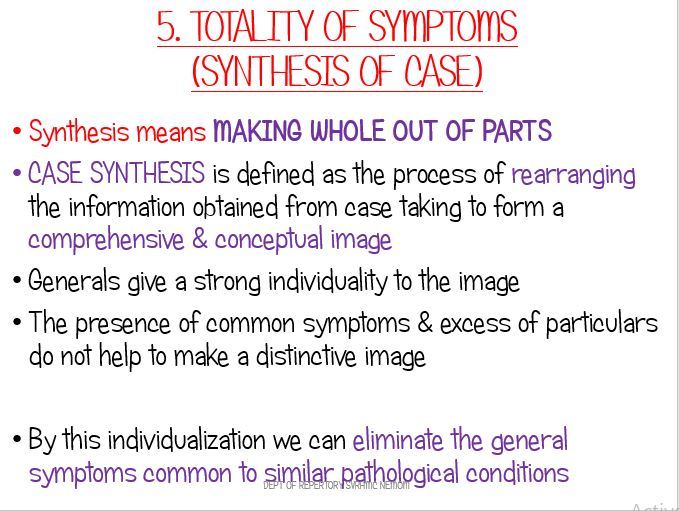
(c) Totality of symptoms or conceptual image of the patient
(d) Reportorial totality
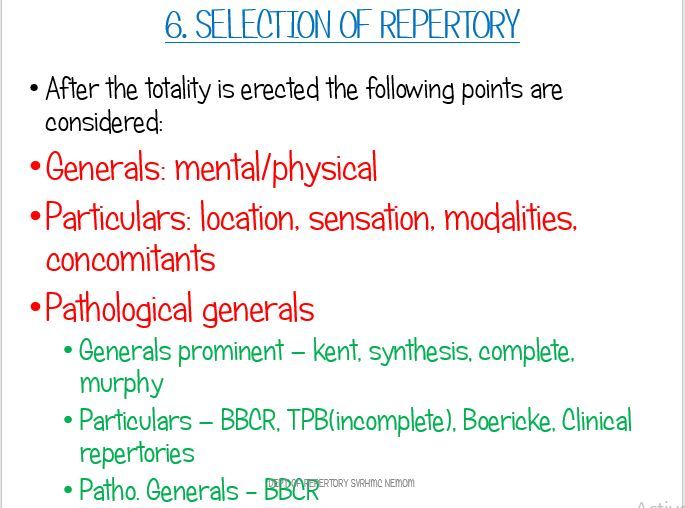
(e) Selection of rubrics
(f) Reportorial technique and results
(g) Reportorial analysis
3. Repertory: definition; Need; Scope and limitations
4. Evolution and Classification of repertories
5. Methods and techniques of repertorisation. Steps of repertorisation
6. Study of Kent’s repertory
(a) History
(b) Philosophical background
(c) Structure
(d) Concept of repertorisation
(e) Adaptability
(f) Scope
(g) Limitations
7. Gradation of remedies by different authors
8. Terms and language of repertories (rubrics) cross references in other repertories and materiamedica
B. Practical or clinical:
1. Record of five cases each of surgery, gynaecology and obstetrics worked out by using Kent’s repertory
2. Rubrics hunting from Kent’s and Boenninghausen repertories
Note: there will be no examination in the subject in third BHMS.
Fourth BHMS.
A. Theory:
1. Conversion of symptoms into rubrics and repertorisation using different repertories
2. Detailed study of Therapeutic Pocket Book and Boger’sBoenninghausens repertory.
3. Comparative study of different repertories like(Kent’s repertory, Boenninghausen therapeutic pocket book and Boger-Boenninghausen characteristic repertories, a synoptic key to materiamedica)
4. Card repertories and other mechanical aide repertories –History, types and use
5. Concordance repertories (Gentry and Knerr)
6. Clinical repertories (Oscar E Boerick, JH Clarke’s repertory, Bell’s Diarrhoea.)
7. Regional repertories – Minton’s Uterus, Berridge’s eye
8. An introduction to modern repertories-(Synthetic, Synthesis and Complete repertory and Murphy’s repertory)
9. Role of computers in repertorisation and different software- RADAR, Hompath, ISIS, Complete Dynamics. Information and Communication Technology (ICT) in homoeopathy through medical apps and softwares. 10. Practice building & concept of digital clinic – how to setup and promote your clinic/hospital
B. Practical or clinical Students shall maintain the following record, namely:-
1. Five acute and five chronic cases (each of medicine, surgery, and obstetrics and gynaecology) using Kent’s repertory
2. Five cases (pertaining to medicine) using Boenninghausen therapeutic pocket book.
3. Five cases (pertaining to medicine) usingBoger-Boenninghausen therapeutic pocketbook.
4. Five cases to be cross checked(integrated medium) on repertories using homoeopathic softwares.
1. THEORY:
1.1 Number of papers-01
1.2 Marks 100
2. Practical including viva voce or oral:
2.1 marks: 100
2.2 distribution of marks: marks
2.2.1 one long case 30
2.2.2 one short case 10
2.2.3 practical record or journal 10
2.2.4 viva voce (oral) 50 -------- Total 100
C. Examination: There will be examination of repertory only in fourth BHMS(not in third BHMS)
IIIrd BHMS - THEORY
1. Repertory: Definition; Need; Scope & Limitations.
2. Classification of Repertories
3. Study of different Repertories (Kent, Boenninghausen, Boger-Boenninghausen): History Philosophical background Structure Concept of repertorization, Adaptability Scope Limitation(s)
4. Gradation of Symptoms by different authors.
5. Methods and techniques of repertorisation. Steps of repertorisation.
6. Terms & Language of repertories (Rubrics) Cross references in other Repertories and Materia Medica.
7. Conversion of symptoms into Rubrics and repertorisation using different repertories.
8. Repertory – its relation with Organon of Medicine and Materia Medica.
9. Case taking and related topics:
9.1. Case taking.
9.2. Difficulties of Case taking, particularly in a Chronic case.
9.3. Types of symptoms, their understanding and importance.
9.4. Importance of Pathology in disease diagnosis & individualization in relation to study of Repertory.
10. Case Processing – -Analysis & Evaluation of symptoms -Miasmatic assessment -Totality of Symptoms/Conceptual image of the patient -Reportorial totality -Selection of rubrics -Repertorial technique and results -Repertorial analysis
Practical/Clinical Work Record of 05 cases each of Surgery, Gynaecology and Obstetrics worked out by using Kent‟s Repertory. Rubrics hunting from Kent‟s & Boenninghausen‟s Repertories.
IVth BHMS
1. Comparative study of different repertories (like Kent‟s Repertory, Boninghausen‟s Therapeutic Pocket Book and Boger-Boninghausen‟s Charactetristic Repertories, A Synoptic Key to Materia Medica).
2. Card Repertories – History, Types & Use.
3. Concordance Repertories (Gentry & Knerr)
4. Clinical Repertories (William Boericke etc.)
5. An introduction to modern Repertories- (Synthetic, Synthesis & Complete Repertory & Murphy‟s Repertory) 6. Regional Repertories
7. Role of Computers in Repertorisation and different softwares.
PRACTICAL Record of:
1. 10 acute & 10 Chronic cases (each of Medicine, Surgery and Obstetrics & Gynaecology) using Kent‟s Repertory
2. 05 cases (pertaining to Medicine) using Boenninghausen‟s Therapeutics Pocket Book.
3. 05 cases (pertaining to Medicine) using Boger-Boenninghausen‟s Characteristics Repertory.
4. 05 cases to be cross checked on Repertories using Homoeopathic softwares.
NEW SCHEME
Repertory
OBJECTIVES
1. Make the students competent enough to take cases in different clinical conditions and situations
2. Successful application of knowledge of repertory in day today clinical practice including management of acute diseases
3. Creating awareness about information and communication technology (ICT) in homoeopathy through medical apps and softwares
INSTRUCTIONS:
I (a) Repertorisationis not the end but the means to arrive at the similimum with the help of material medica based on sound knowledge of homoeopathic philosophy;
(b) Homoeopathic materiamedica is an encyclopedia of symptoms. No mind can memorize all the symptoms of all the drugs with their gradations;
(c) The repertory is an index and catalogue of the symptoms of the materiamedica nearly arranged in a practical or clinical form with the relative gradation of drugs, which facilitates quick selection of indicated remedy and it may be difficult to practise homoeopathy without the aid of repertories.
II (a) each repertory has been compiled on distinct philosophical base, which determines the structure;
(b) In order to explore and derive full advantage of each repertory, it is important to grasp thoroughly its conceptual base and construction and this will help students to learn scope, limitations and adaptability of each repertory.
Third BHMS
A. Theory:
1. Case taking and related topics:
(a) Case taking
(b) Difficulties of case taking, particularly in a chronic case.
(c) Types of symptoms, their understanding and importance
(d) Importance of pathology in disease diagnosis and individualisation in relation to study of repertory. Correlation of other clinical and nonclinical subjects in case taking and repertorisation. Repertory- its relation with organon of medicine and materiamedica
(e) Case taking in different clinical conditions and situations
(f) Reportorial approach in case taking
(g) Standardised case record. Different methods of record keeping
(h) Application of knowledge of repertory in acute diseases
2. Case processing
(a) Analysis and evaluation of symptoms
(b) Miasmatic assessment
(c) Totality of symptoms or conceptual image of the patient
(d) Reportorial totality
(e) Selection of rubrics
(f) Reportorial technique and results
(g) Reportorial analysis
3. Repertory: definition; Need; Scope and limitations
4. Evolution and Classification of repertories
5. Methods and techniques of repertorisation. Steps of repertorisation
6. Study of Kent’s repertory
(a) History
(b) Philosophical background
(c) Structure
(d) Concept of repertorisation
(e) Adaptability
(f) Scope
(g) Limitations
7. Gradation of remedies by different authors
8. Terms and language of repertories (rubrics) cross references in other repertories and materiamedica
B. Practical or clinical:
1. Record of five cases each of surgery, gynaecology and obstetrics worked out by using Kent’s repertory
2. Rubrics hunting from Kent’s and Boenninghausen repertories
Note: there will be no examination in the subject in third BHMS.
Fourth BHMS.
A. Theory:
1. Conversion of symptoms into rubrics and repertorisation using different repertories
2. Detailed study of Therapeutic Pocket Book and Boger’sBoenninghausens repertory.
3. Comparative study of different repertories like(Kent’s repertory, Boenninghausen therapeutic pocket book and Boger-Boenninghausen characteristic repertories, a synoptic key to materiamedica)
4. Card repertories and other mechanical aide repertories –History, types and use
5. Concordance repertories (Gentry and Knerr)
6. Clinical repertories (Oscar E Boerick, JH Clarke’s repertory, Bell’s Diarrhoea.)
7. Regional repertories – Minton’s Uterus, Berridge’s eye
8. An introduction to modern repertories-(Synthetic, Synthesis and Complete repertory and Murphy’s repertory)
9. Role of computers in repertorisation and different software- RADAR, Hompath, ISIS, Complete Dynamics. Information and Communication Technology (ICT) in homoeopathy through medical apps and softwares. 10. Practice building & concept of digital clinic – how to setup and promote your clinic/hospital
B. Practical or clinical Students shall maintain the following record, namely:-
1. Five acute and five chronic cases (each of medicine, surgery, and obstetrics and gynaecology) using Kent’s repertory
2. Five cases (pertaining to medicine) using Boenninghausen therapeutic pocket book.
3. Five cases (pertaining to medicine) usingBoger-Boenninghausen therapeutic pocketbook.
4. Five cases to be cross checked(integrated medium) on repertories using homoeopathic softwares.
1. THEORY:
1.1 Number of papers-01
1.2 Marks 100
2. Practical including viva voce or oral:
2.1 marks: 100
2.2 distribution of marks: marks
2.2.1 one long case 30
2.2.2 one short case 10
2.2.3 practical record or journal 10
2.2.4 viva voce (oral) 50 -------- Total 100
C. Examination: There will be examination of repertory only in fourth BHMS(not in third BHMS)
CBDC SYLLABUS
This is a generic article you can use for adding article content / subjects on your website.
Read MoreNOTES FOR EXAM
INTRODUCTION
INTRODUCTION TO REPERTORY - RELATION WITH OTHER SUBJECTS; PURPOSE
HISTORY OF REPERTORIES
It was really surprising that the third and later American editions of Kent’s Repertory had many printing mistakes and these errors had not been rectified by Dr. Kent. Was it that Dr. Kent never had the chance to correct these errors or was it corrected in later editions ???
LET'S HAVE A HISTORICAL TOUR, NOT ONLY KENT.... BUT TPB AND BBCR TOO !!!!
HISTORY OF EVOLUTON OF REPERTORY NOTES
HISTORY OF KENT'S REPERTORY - NOTES.pdf
KENT REPERTORY - HISTORY PART 1.pdf
KENT REPERTORY - HISTORY PART 2.pdf
TPB - HISTORY & PHILOSOPHY.pdf
BOGER REPERTORY - HISTORY & INTRODUCTION.pdf
BOGER REPERTORY - HISTORY & INTRODUCTION II.pdf
COMPARISON OF REPERTORIES
Every Repertory has got its own advantages & disadvantages. Each one follows a definite plan and construction and is based on a sound philosophy. Adequate acquaintance with the repertory is needed to put it to maximum use..
HOW TO GET ACQUAINTANCE WITH REPERTORIES ???
COMPARATIVE STUDY OF RUBRICS IS A WAY TO IT....
TPB - HISTORY & PHILOSOPHY.pdf
BOGER REPERTORY - HISTORY & INTRODUCTION.pdf
BOGER REPERTORY - HISTORY & INTRODUCTION II.pdf
KENT REPERTORY - HISTORY PART 1.pdf
CASE TAKING
 For the determination of a homeopathic remedy, the physician or therapist first needs to know the case history. Is it so simple? This process requires a great deal of mental effort, a highly penetrating insight into the individual patient, and a massive amount of studying..
For the determination of a homeopathic remedy, the physician or therapist first needs to know the case history. Is it so simple? This process requires a great deal of mental effort, a highly penetrating insight into the individual patient, and a massive amount of studying..
CASE TAKING $ INTRODUCTION 2020 II.pdf
CASE TAKING $ INTRODUCTION 2020 III.pdf
DIFFICULTIES IN CHHRONIC CASE TAKING .pdf
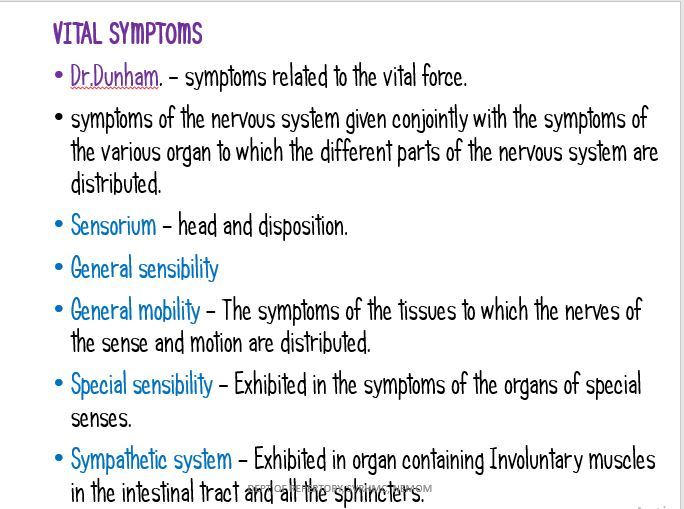
SYMPTOMATOLOGY
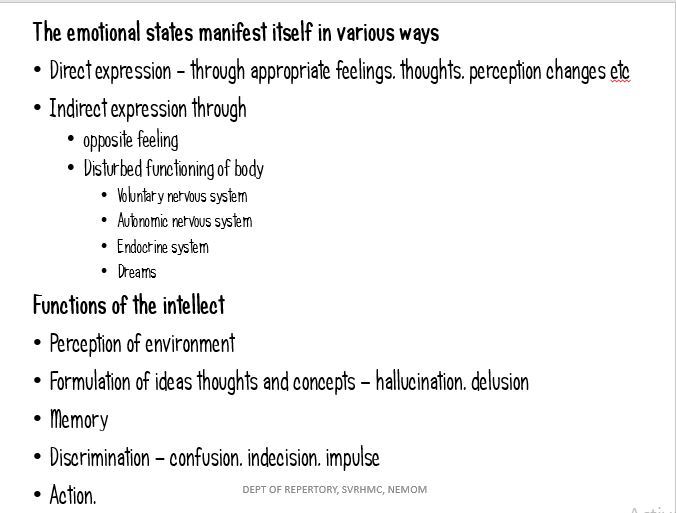
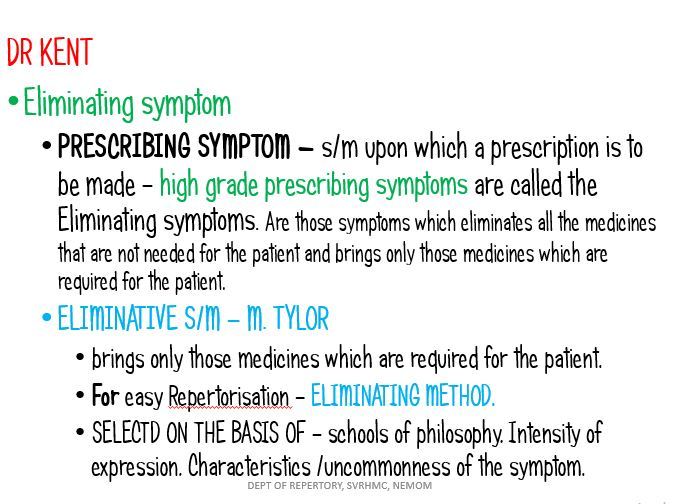
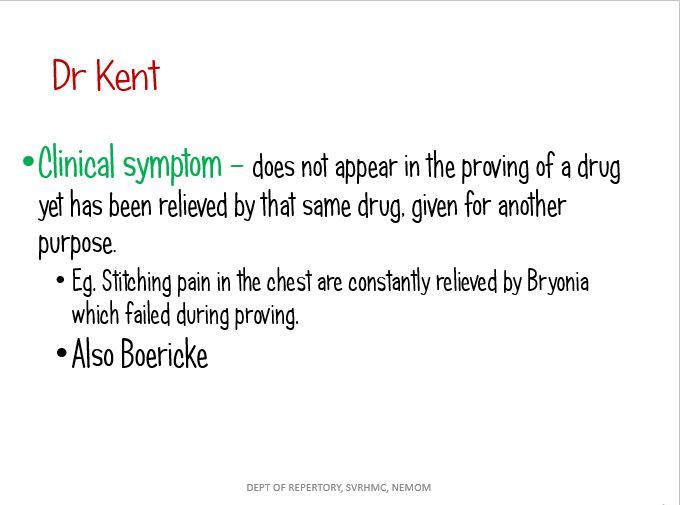
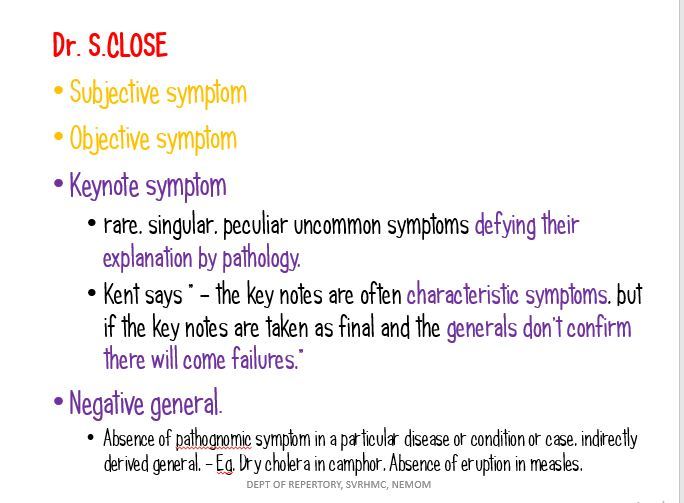
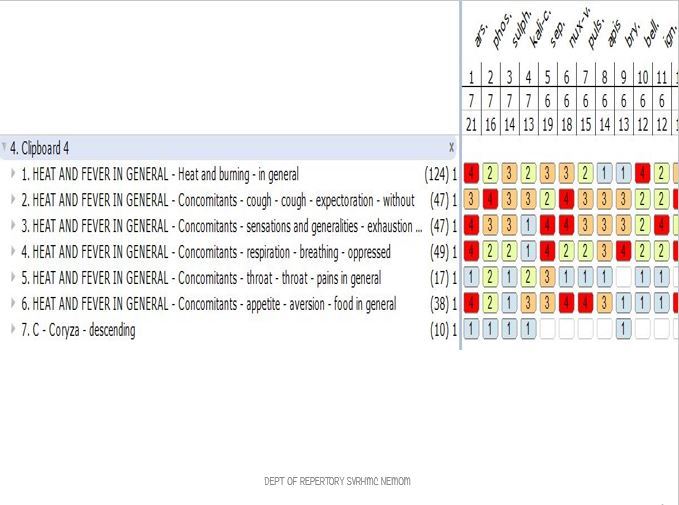
STEPS TO REPERTORISATION
RULES FOR REPERTORIAL RESULT ANALYSIS
" Know the rules well, so you can break them effectively"... Here are some rules for breaking your Repertorial Result!!!

METHODS & TECHNIQUES OF REPERTORISATION
REPERTORISATION is a technique of finding out the most similar medicine of a case with help of a repertory following some special mathematical calculation. Then HOW TO DO IT??? Here is the answer......
 METHODS & TECHNIQUE OF REPERTORISATION.pdf
METHODS & TECHNIQUE OF REPERTORISATION.pdf
CLASSIFICATION OF REPERTORIES
 Repertories have come a long way since the time of Dr. Hahnemann with more than 200 repertories available as of today.
Repertories have come a long way since the time of Dr. Hahnemann with more than 200 repertories available as of today.
Each of them hold importance in their own specific way and the selection of the repertory ultimately lies on the acumen of the homeopath
So there comes the need for CLASSIFICATION OF REPERTORIES......
REPERTORY - MERITS & DEMERITS
ADVANTAGES AND LIMITATIONS OF REPERTORY
Courtesy: www.homeobook.com
Repertory is an index of homoeopathic materia medica which is full of information collected from toxicology, drug proving and clinical experiences.
The process of repertorisation is essentially an elimination, which starts with a broad choice and slowly narrows down the field, giving us adequate small group of medicine, so that the final selection is made easier with the help of further reference to the materia medica.
NEED/ SCOPE OF REPERTORY
1. To avoid routinism.
2.It teaches by gradation the relative importance of various medicines
3.To select similimum quickly.
4. Helps to find out complete symptom.
5. It promotes discovery of medicine which one had not thought of
6. Second prescription and related remedies
7. Its constant use makes the physician efficient.
8.. It help the physician to ask intelligent questions.
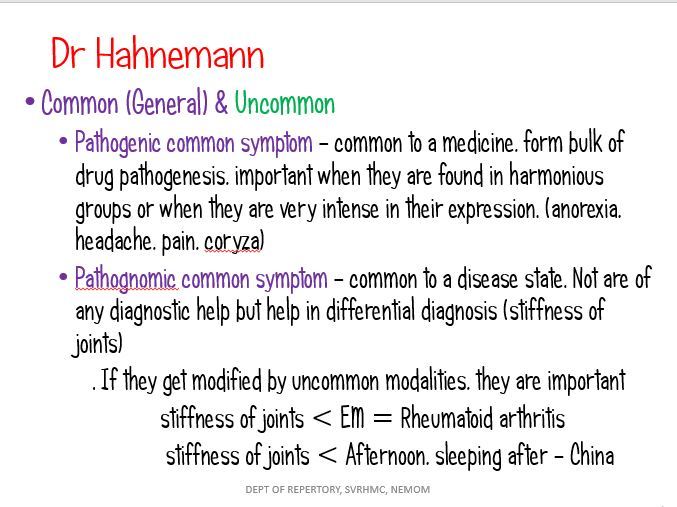
9. Repertory teaches us to be careful about those symptoms belonging to the disease [common symptoms] and to consider only those symptoms which lie outside the disease [uncommon symptoms of the disease]
10. It help the study of Materia medica and comparative study of drugs.
11.To recall
LIMITATIONS OF REPERTORY
Courtesy: www.homeobook.com
Repertory is an index of homoeopathic materia medica which is full of information collected from toxicology, drug proving and clinical experiences.
The process of repertorisation is essentially an elimination, which starts with a broad choice and slowly narrows down the field, giving us adequate small group of medicine, so that the final selection is made easier with the help of further reference to the materia medica.
NEED/ SCOPE OF REPERTORY
1. To avoid routinism.
2.It teaches by gradation the relative importance of various medicines
3.To select similimum quickly.
4. Helps to find out complete symptom.
5. It promotes discovery of medicine which one had not thought of
6. Second prescription and related remedies
7. Its constant use makes the physician efficient.
8.. It help the physician to ask intelligent questions.
9. Repertory teaches us to be careful about those symptoms belonging to the disease [common symptoms] and to consider only those symptoms which lie outside the disease [uncommon symptoms of the disease]
10. It help the study of Materia medica and comparative study of drugs.
11.To recall
LIMITATIONS OF REPERTORY
- Repertory is basically an index, never suggest a final choice.
- Different repertories have different philosophy and construction.
- New additions to materiamedica cannot be accommodated in repertory.
- Many rubrics are not represented well.
- No guidance about potency, dose and repetition.
- Nosodes and sarcodes not represented well.
- If the physician makes mistakes in interpretation, and just counting the symptoms and markes, he will fail.
- Use of repertory cannot be independent of knowledge of materia medica, organon or clinical subjects.
EVOLUTION OF REPERTORY
Important events in evolution of repertories
Courtesy: www.homeobook.com
Courtesy: www.homeobook.com
- Fragmenta de viribus : 1805 in latin 4239 pages include 27 remedies
- Glazor, first alphabetical repertory : 1833
- Weber,repertory of purely pathognomic effects : 1833
- Jahr’s repertory : 1835 in German
- Lafflie- A Homeopathic repertory of symptamatology : 1843 ( 1st French repertory- Hahnemann died this year)
- Clopaer Muller : 1848
- Hempel’s repertory : 1847
- Brayant : 1851
- Hempel’s complete repertory : 1853
- Lippe’s repertory of comparative materiamedica : 1854 144pages
- Lippe’s repertory of more characteristics : 1879 322 pages
- Cipher’s repertory : 1859
- Huge’s cyclopedia of drug pathogenesy : 1892
- Morgan’s urinary organs : 1899
- JH Clark’s clinical repertory : 1904
- Minton’s uterus : 1906
- Nash repertory : 1906
- Raue’s special pathology : 1906
- Boricks repertory : 1927
- Bell’s Diarrhoea : 1820
- Berridge’s eye : 1873
- Guernesy’s desire & aversions : 1873
- Guernesy’s hemorrhoids : 1880
- Moon phase by Boger : 1931
- Synoptic Key by Boger : 1931
- Sensation as if by H.A.Robert : 1937
- Rheumatic remedies by H.A.Robert : 1945
- Repertory of fever by H.C.Allen : 1880
- Repertory of Intermittent fever by W.A.Allen : 1883
- First Indian Repertory Augustus Muller : 1885
- English translation of anti psorics by Boger : 1900
- T.F.Allen Symptom register : 1880
- Hering’s Analytical repertory : 1881
- Gentry’s concordances : 1890
- Kneer repertory : 1896
- N.M.Choudary ‘s material medica with repertory : 1929
- In 1838 the first English language repertory was published by C.M.Hering
- First computer repertory : Melanic in 1979
- INDIAN SOFT WARE PROGRAMME
- Kentopath _ Pune
- CIRH – Kerala
- Hompath _ Dr. Jawahar shaw
- Organon _ 96 (Dr.Dixit,case taking only )
- Cara _ Sanjeevani creations
- FOREIGN SOFT WARE PROGRAMMES
- Lamina _ Australia.
- Cara _ Computer aided repertory analysis.
- VEs _ Vithoulkas expert system.
- Radar _ Rapid aid to drug aimed research.
- KBex _ Knowledge based expert system.
- 1987. Kent’s Repertorium General by Kunzli.
- 1987. Synthesis by Dr.Fredericke schroyens based on RADAR.
- 1996. Comparative repertory of Homoeopathic MM by Dockx & Kokelenberg.
- 1993. Homoeopathic Medical Repertory by Robin Murphy.
- 1996. Complete Repertory by Roger Von Zandervoort.
- 2004. Repertorium Universalice by Roger Von Zandervoort
TPB
TPB - HISTORY & PHILOSOPHY.pdf
Courtesy: www.homeobook.com
Name of the book: BOENNINGHAUSEN’S THERAPEUTIC POCKET BOOK
Full Name of the book: Boenninghausen’s Therapeutic Pocket Book for Homoeopathic Physicians to Use at the Bedside and in the Study of the Materia Medica
First Edition : 1846
Editor : T.F.Allen
Introduction : Dr.H.A.Roberts & Dr. Annie C Wilson
Publisher : B.Jain Publishers Pvt.Ltd , New Delhi
Printer : J.J. Offset Printers. New Delhi
Contents:
Part I
- Preface
- Life History of Boenninghausen
- Introduction
Part II
- Repertory Proper
- Index
Introduction
- Repertory Uses
- The art of physician in taking the case
- The philosophic Background
- Construction of the Repertory
- Introduction to different Chapters
- Mind and intellect
- Parts of the Body and Organs
- Sensations and complaints
- Sleep and Dreams
- Fever
- Alterations of State of Health
- Relationships of Remedies
- Limitations of Repertory
- Use of the Analysis
- Preface to the New American Edition
- Boenninghausen’s Original Preface
PART I
- Preface by Dr. T.F. Allen - In the preface Dr. T.F. Allen says that his aim is to demonstrate the sound philosophy and practical application of this work to such state as the physician meets in everyday practice.
- Life History of Boenninghausen - He was born in Netherlands. There is a controversy about the birth year of Boenninghausen, according to Lippe it is 1777. But in the beginning of the chapter the year given is 1785. H.A. Roberts and Annie .C. Wilson gives a brief sketch of Boenninghausen’s life and they show how a lawyer turned to an expert Homoeopath. It was Dr. Weihe who influenced Boenninghausen by rescuing him from the purulent tuberculosis with the help of Pulsatilla.
Authors give works of Boenninghausen in their order of appearance. They are:
- The cure of cholera and its preventives 1831
- Repertory of Antipsoric Medicines 1832
- Summary View of the Chief Sphere of Operation of the Antipsoric Remedies and of their characteristic Peculiarities, as an appendix to their Repertory 1833
- An attempt at a Homoeopahtic Therapy of Intermittent fever 1833
- Contributions to a Knowledge of the Peculiarities of Homoeopahtic Remedies1833
- Homoeopahtic Diet and a Complete Image of a Disease 1833
- Homoeopathy a Manual for the Non- Medical Public1834
- Repertory of Medicines which are not Antipsoric 1835
- Attempt at showing the Relative Kinship of Homoeopahtic Medicines 1836
- Therapeutic manual for Homoeopahtic Physicians, for use at the sick bed and in the study of the Materia Medica Pura 1846
- Brief Instructions for Non- Physicians as to the Prevention and Cure of Cholera 1849
- The two sides of Human body and Relationships. Homoeopahtic studies 1853
- The Homoeopahtic domestic Physician in Brief Therapeutic Diagnosis. An attempt 1853
- The Homoeopahtic treatment of Whooping Cough in its Various Forms 1860
- The Aphorisms of Hippocrates with Notes by a Homoeopath 1863
- Attempt at a Homoeopathic Therapy of Intermittent and Other Fevers, especially for would- be Homoeopaths 1864
- Philosophic Background
BTP is based upon the following fundamental concepts:-
- Doctrine of analogy and doctrine of grand generalisation
- Doctrine of concomitant
- Evaluation of Remedies
- Concordances
Doctrine of Analogy/Doctrine of Grand Generalization
To make a symptom complete, the local modalities and sensations pertaining to one part should be applicable to other parts; in case modalities and sensations are not experienced by the patient or unnoticed by the Physician. Thus he raised local symptoms to a general level which could be used for the whole person. Thus all those modalities which are noticed in one part, but missing in any other part should be taken as an expression of the whole person.
Doctrine of Concomitant
Boenninghausen, identified in each case a group of symptoms along with the main complaint; such symptoms were generally overlooked by the patient, and un noticed by the physician. They appear to be unrelated to the main complaint; but are quite crucial in individualizing the case as well as the remedy.
Evaluation of Remedies
Boenninghausen was the first to grade the remedies. He noticed that there is difference in the frequency and intensity in the appearance of symptoms in provers.
He graded the remedies into 5 grades – or marks.
He used different typography to represent these different grades of remedies.
CAPITAL - I Grade (5 marks) - Proved (Recorded), Reproved (confirmed), Clinically verified.
Bold - II Grade (4 marks) - Proved (less than the1st grade), Reproved, (Confirmed) occasionally Verified.
Italics - III Grade (3 marks) - Now and then a prover brings out symptom, Not confirmed, But verified Clinically
Roman - IV Grade ( 2 marks) - Only clinically verified
(Roman) in paren- thesis - V Grade ( One mark ) - Not confirmed, Not verified, doubtful remedies, But proved.
Concordances
He discusses the relationship of remedies; under headings – mind,locality, sensation, glands, bones skin, sleep and dreams, blood, circulation, fever, aggravation, other remedies, antidotes and inimical.
Plan and Construction
The whole book can be divided into 3 components of a symptom – Location, sensation, and modalities. However concomitants are found scattered. Plan of Allen’s modified edition:-
- I Mind and Intellect
- II PARTS OF THE BODY
- III. Sensations and Complaints
- 1. Sensations — In general
- 2. Sensations — Glands
- 3. Sensations — Bones
- 4. Sensations — Skin
- IV Sleep and Dreams
- V Fever
- VI. Modalities
- VII Relationship of remedies.
Mind and Intellect: Mind Chapter contains 18 rubrics and Intellect Chapter contains 17 rubrics. In order to clarify the use of the book he simplified the number of rubrics as far as possible. Boenninghausen based his work on the concept of the whole man, placing the balance of the emphasis on the value of concomitants and the modalities. It was not his intention to reflect the whole man through his mental reactions, as they may be difficult to get. Even though this chapter contains only 35 rubrics, the aggravation chapters include 17 rubrics related to emotional excitement or state.
Though he has given emphasis to the Concomitants in case taking, the concomitants of mental symptoms are given under a single rubric “ Drugs which have concomitants of Mental Symptoms.”Part 2
Parts of the body and organs
This section of the book follows in general the anatomical schema used by Hahnemann. T.F. Allen added many of the rubrics in the eye section. He also used an idea of combining Boenninghausen’s Repertory of the Sides of the Body with the original Pocket Book.
Part 3 Sensations:
It include rubrics related to various Complaints also, hence Boger has renamed this chapter as Sensations and Complaints in General.
Part 4 Sleep:
This chapter include sleep in general , positions during sleep, and dreams. The last two are given as separate chapters.
Part 5 Fever
This chapter includes
- Circulation
- Chilliness in general
- Heat
- Coldness in general
- Shivering in general
- Sweat in general
- Compound Fevers in General
Though Circulation is given as a separate chapter it is included under the Fever Chapter.
The old Edition contain these seven sub- sections.
- Circulation
- Chill
- Heat
- Sweat
- Compound fevers
- Concomitants of Fever
- Febrile Symptoms – Left side, Right side
Part 6 Alterations of the state of Health
Aggravation: First the time modalities are given, specific time modalities are not given.
Amelioration: Some rubrics does not contain medicines, their reference is given in brackets.
They are asked to refer in the Aggravation chapter- among the rubrics with opposite meaning.
Part 7 Relationship of remedies
In the earlier editions the name of this chapter was Concordance of Remedies.
This chapter contains relation ship of 141 Medicines.
1. It can be used for studying the relationship of remedies at various levels- mind, parts, sensation, modalities 2. It is helpful for finding out the second prescription
3. In certain cases a deep acting medicine cannot be given even though indicated, so as to avoid unwanted precipitation of adverse symptoms.
Advantage of TPB
- It is based upon the concept of complete symptom- location, sensation, modality, and concomitant.
- It follows more or less an anatomical schema which is helpful for finding the rubrics.
- By applying the ‘Doctrine of analogy’ rubric can be completed, even though there is lack of any of the four parts of the symptom.
- Five gradations of medicines are one of the unique contribution of Boenninghausen.
- This repertory has given more importance to concomitant symptoms than Kent’s repertory.
- Modalities are given under separate section. Ameliorations are also given more importance than Kent’s repertory.
- This repertory is useful in working out cases which are full of particulars and which contain few mental generals and physical generals. Cases manifested by pathological changes and objective symptoms can better dealt by BTPB.
- Rubrics are given in simple language.
- Chapter ‘relationship of remedies’ is helpful for finding the second prescription.
- The sides of the body are given importance, they are mentioned in location chapter.
- The extremities are divided into upper and lower which is helpful for finding the rubrics very easily.
Disadvantage of BTP
- It deals with only 342 remedies. Boenninghausen’s original edition contained 126 remedies. Allen dropped 4 remedies (Angustra, Magnetis Polus Articus, Magnetis Polus Australius, Magnetis Poli Umbo) and added 220 remedies.
- The rubrics given in the book are not many in number.
- Many of the rubrics lack important medicines-desire for salt – Natrum mur is not mentioned.
- Mind section contains only 18 rubrics under ‘mind’ and 17 rubrics under intellect. These rubrics are too general and can only be used as reference.
- The concept that a symptom that refers to a part may be predicated of the whole man (Doctrine of analogy) is not correct under many circumstances.
- Though prime importance is given to the concomitants there is no separate chapter for them.
- Even though this book has undergone many modifications and editions there are many defects in the construction and compilation.- Internal head ends on page 26 , again starts on page 29. – External head ends on page 29 , again starts on page 30.
- Rubrics that might have been placed under ‘ sensations’ are given under ‘parts of the body’- Toothache under teeth, stopped feeling in ears.
- There is no fixed arrangements of rubrics.
- The relationship section deals with only 141 remedies.
- There are many misplaced rubrics- Vertigo-is given in intellect,Perineum is given in chapter stool
- Different sensations are given specifically , but in practice many patients do not specify their sensations.
- This book lacks information about Sarcodes and Nosodes.
BOENNINGHAUSEN TOTALITY

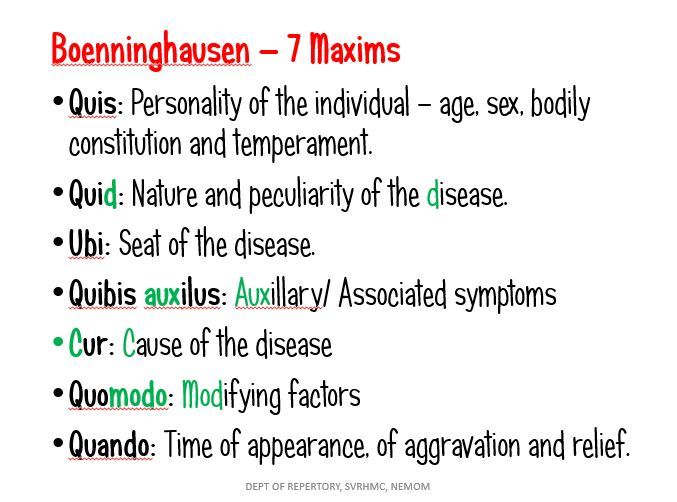
(7 Maxims of Boenninghausen)
In his concept totality of symptoms comprises following seven points.
Quis - Personality, the individuality
Quid - Disease, its nature and peculiarity
Ubi - Seat of the disease
Quibus auxilis - Accompanying symptoms.
Cur - Cause of disease
Quomodo - Modification, agg. and amel.
Quando - Time
Philosophical background of Boenninghausen’s repertory rests on the following.
(Bed rock of TPB / Doctrine of TPB)
1. Doctrine of Analogy
2. Doctrine of concomitance
3. Evaluation of remedies
4. Concordance
DOCTRINE OF ANALOGY:
According to Boenninghausen one can make a complete symptom combining the scattered symptoms by making use of analogy. To complete a symptom local maladies and sensations pertaining to one part should also be applied to other parts. Thus he raised local symptoms to a general level which could be used for the whole person this is called DOCTORINE OF GRAND GENERALIZATION. He also evolved the concept that ‘what is true to the part is also true to the whole person’. Boenninghausen’s approach was that proving are not complete and can never be really complete. He says that to make things comparatively more complete, so as to make the best of what can be found out
DOCTRINE OF CONCOMITANT:
The word concomitant means existing or occurring together; or attendant. They are the UNREASONABLE ATTENDANTS of the case. Boenninghausen identified in each case a group of symptoms which have no relation to the leading symptom from the standpoint of theoretical pathology, yet they have actual relationship with the case in that they exist in same person at the same time. Concomitant is the differentiating factor in any case. The foundation of the TPB lies in it.
EVALUATION OF REMEDIES: – Boenning Hausen was the first to grade the remedies, there are 5 gradings
CAPITALS- 5 marks FIRST GRADE
BOLD 4 marks SECOND GRADE
ITALICS 3 marks THIRD GRADE
ROMAN 2 marks FOURTH GRADE
ROMAN ( PARANTHESIS) 1 mark FIFTH GRADE
This gradation is based on frequency and intensity of the appearance of symptom in provers.
5 marks Symptom frequent, confirmed and verified
1 mark Symptom not verified, not confirmed
CONCORDANCE:
In the earlier edition the heading of TOB's Relationship chapter was CONCORDANCE OF REMEDIES. ( In the earliest edition boenninghausen named it as ENIGMA meaning PUZZLE. Later boenninghausen himself changed it to concordance) Allen changed it to relationship of remedies. This chapter is divided into sections, each begin with a section devoted to a remedy in alphabetical order.
Each of these remedy section is subdivided into rubric Mind, Localities, Sensation, Glands, Bones, Skin, Sleep and Dreams, Blood; Circulation and Fever, Aggravation: Time and circumstances, Other remedies, Antidotes, Injurious. Other remedies mean general relationship of remedies. Other remedies also cover these symptoms which do not into the above said rubrics.
KENT REPERTORY
BBCR
CONCORDANCE REPERTORY
 The word concordance means harmony, synchronization; arrangement in alphabetical order of important words etc.. and this word was first of all used by Boenninghausen in homoeopathic literature. What is its relation with Repertory??
The word concordance means harmony, synchronization; arrangement in alphabetical order of important words etc.. and this word was first of all used by Boenninghausen in homoeopathic literature. What is its relation with Repertory??
CLINICAL & REGIONAL REPERTORY
 There are many repertories which are time proven but few of them become popular and remain in mind of a physician. Its immense usefulness in certain cases cannot be ruled out...
There are many repertories which are time proven but few of them become popular and remain in mind of a physician. Its immense usefulness in certain cases cannot be ruled out...
MODERN REPERTORIES
SOFTWARE

APHORISMS
HAHNEMANN & REPERTORY
RECORD KEEPING :
- In foot note to aphorism 153 he mentioned the Repertory of Jahr & Boenninghausen
- Case taking : $ 83-104
- Chronic case taking : $ 94- 98
- Acute case taking : $ 99-102
- When patient coming directly : $ 83-90
- When patient coming from other physicians : $ 91-93
- A concise idea about case taking : $ 5
- General directions in case taking : $ 83-93
- Incomplete information can be made complete : $ 86
- When the case taking come to a dead end : $ 88
- Nature of consultation : $ 84
- Every new expression in fresh line : $ 85
- Don’ts in case taking : $ 87
- Discounting symptoms : $ 91
- Case taking in fulminate acute disease : $ 92
- Exaggerating patients : $ 96
- Modest patients : $ 97
- Epidemic diseases : $ 100
- Acute exacerbation : $ 215-216
- Mental disease : $ 208-230
- Leading questions : $ 88
- Classification of diseases : $ 72-81
- Types of acute disease : $ 73
- Types of chronic diseases : $ 74
- Artificial chronic diseases : $ 75
- False chronic diseases : $ 77
- True natural chronic diseases : $ 78
- Record keeping : $ 104
- One sided disease : $ 173
- Local maladies : $ 185
- Intermittent diseases : $ 231
- Alternating diseases : $ 232
- Intermittent fevers : $ 235
RECORD KEEPING :
- Aphorism 104
- Dr.Boenninghausen was the first to publish the case histories recorded by Hahnemann
- Hering recommend loose sheets instead of bound journal
- Hering always notes the weather condition and position of moon in each visit.
- Lutzes firstly recommended ingenious filling slip system.
- Without case records you are at see without a compass or rudder : Kent.J.T
MODERN REPERTORIES
Courtesy: www.homeobook.com
SYNTHETIC REPERTORY
Full name : Synthetic Repertory
Author : This was originally published by G.Haug Verlag Gmbh & Co. & improved on 1982 by Barthel & Will Klunker. It was basically an extension of Kent’s Repertory.
Barthel : Vol 1&2
Klunker : Vol 3
1594 medicines,6 chapters
Author used 16 authorities
138 new rubrics than Kent denoted by * asterisk
Gradations :
CAPITAL UNDERLINED : 4 marks
CAPITAL : 3 marks
Bold : 2 marks
roman : 1 marks
Full name : Homeopathic Medical Repertory
Author : Robin Murphy ND
Base : All Kent + A part of Kneer repertory
SYNTHESIS REPERTORY
Full name : Repertorium homeopathicum Syntheticum
Editor : Frederick Schroyens
Base : 6th edition of Kent’s Repertory
First edition : 1987 RADAR
Book version : 1995
Indian edition : 1996
9th version of RADAR : 2004
RADAR was first developed as research project at University of Namur,Belgium under supervision of Jean Fichefet who is a professor of Maths ,his sympathetic reaction after the homeopathic cure of his son was the begning of everything.
Gradations :
KENT’S REPERTORIUM GENERAL
Full name : Kent’s Repertorium General
Author : Jose Kunzhli having 40 years of clinical experience
First edition : 1987 in German
English edition : 1987
72 sources, 689 medicines, 98 more remedies than Kent
Red dots are famous in homeopathic circle – therapeutic efficacy of a drug or therapeutic importance of a rubric.
He omitted 7 drugs in Kent
The work was compiled & edited by Michael barthel with the able assistance of Charlotte Barthel & Ilse Seider
COMPLETE REPERTORY
Author : Roger Von Zandvoort
The initial version came out as a database file for use with Kent homeopathic associates Mac repertory. After the death of Jost Kunzli, the supervision work was taken up by Dr. Dario Spinedi.
Preface by Dr. Dario Spinedi.
First editions : 1996
Base : 1st . 3rd and 6th edition of Kent’s repertory
SYNTHETIC REPERTORY
Full name : Synthetic Repertory
Author : This was originally published by G.Haug Verlag Gmbh & Co. & improved on 1982 by Barthel & Will Klunker. It was basically an extension of Kent’s Repertory.
Barthel : Vol 1&2
Klunker : Vol 3
- First edition : 1973
- Second edition : 1982
- Indian edition : 1987
- Third edition : 1993
1594 medicines,6 chapters
Author used 16 authorities
138 new rubrics than Kent denoted by * asterisk
Gradations :
CAPITAL UNDERLINED : 4 marks
CAPITAL : 3 marks
Bold : 2 marks
roman : 1 marks
- no italics in gradations
- In mind 600 rubrics,33 cross references , 18 rubrics of Kent are missing in Mind chapter
- Appetite rubric is not in this repertory
- Remedies are printed under each rubric and not after the rubrics.
- For practical reasons Kent’s abbreviations have been Kept
- The pages of the repertory are divided into two by a middle line – both divisions are counted as separate pages.
- This repertory mention for the first time the exact source of symptoms or drugs added to Kent’s repertory. And uses a numbering system
Full name : Homeopathic Medical Repertory
Author : Robin Murphy ND
Base : All Kent + A part of Kneer repertory
- First edition : 1993
- Indian edition : 1994
- Second edition : 1996
- Third edition 2010
- BOLD CAPITAL
- Bold Italics
- roman
- 67+3 : 70 chapters in new editions
- 1851 drugs , from 55 sources
- 39,000 new rubrics, 2 lakh additions
- Alphabetical repertory
- Missing chapters compared to Kent - Expectoration, Prostate gland, Urethra
- Kent’s extremities is divided into 12 chapters in Murphy
SYNTHESIS REPERTORY
Full name : Repertorium homeopathicum Syntheticum
Editor : Frederick Schroyens
Base : 6th edition of Kent’s Repertory
First edition : 1987 RADAR
Book version : 1995
Indian edition : 1996
9th version of RADAR : 2004
RADAR was first developed as research project at University of Namur,Belgium under supervision of Jean Fichefet who is a professor of Maths ,his sympathetic reaction after the homeopathic cure of his son was the begning of everything.
Gradations :
- BOLD CAPITAL
- Bold roman
- Italics
- roman
- RED BOLD CAPITAL UNDERLINED
- RED BOLD CAPITAL
- Blue italics
- roman
- 3712 medicines, from 390 sources, 2,35,000 additions, 60,100 new rubrics
- International time table 0-24hr has been followed
- Aggravations are not mentioned except in Generalities Food & Drinks
- Aggravation of a particular food means also the ailments from having that particular food.
- More readable symptom format
- Repeatedly checked additions
- New standard list of remedy abbreviations
- New standard list of author abbreviations
- Chapter Eye & Vision- thoroughly revised by Edwared Kondrot-a homeopathic ophthalmologist
KENT’S REPERTORIUM GENERAL
Full name : Kent’s Repertorium General
Author : Jose Kunzhli having 40 years of clinical experience
First edition : 1987 in German
English edition : 1987
72 sources, 689 medicines, 98 more remedies than Kent
Red dots are famous in homeopathic circle – therapeutic efficacy of a drug or therapeutic importance of a rubric.
He omitted 7 drugs in Kent
The work was compiled & edited by Michael barthel with the able assistance of Charlotte Barthel & Ilse Seider
COMPLETE REPERTORY
Author : Roger Von Zandvoort
The initial version came out as a database file for use with Kent homeopathic associates Mac repertory. After the death of Jost Kunzli, the supervision work was taken up by Dr. Dario Spinedi.
Preface by Dr. Dario Spinedi.
First editions : 1996
Base : 1st . 3rd and 6th edition of Kent’s repertory
- 5,15,000 additions
- 41 chapters, Dreams in Mind
- Three volumes or All in one volume
- CAPITAL BOLD UNDERLINED
- CAPITAL BOLD
- Bold italics
- Roman
- Number of medicines : 2171
- Author identification numbers are based on chronology , based on the dates of the listed authors first published their work.
- Author : Dr.Sivaraman in 1994
- Gradations :
- BOLD CAPITAL
- Bold Italics
- roman
- Sub rubrics are printed in bold roman to avoid confusion
- Time changed as 12 am –to 12 night
- 12 pm – to 12 noon
- He prepared a separate book on word index and also a book on 1st grade remedies.
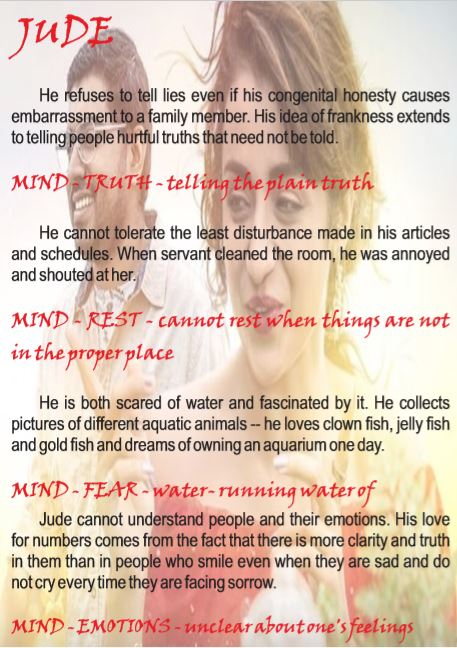
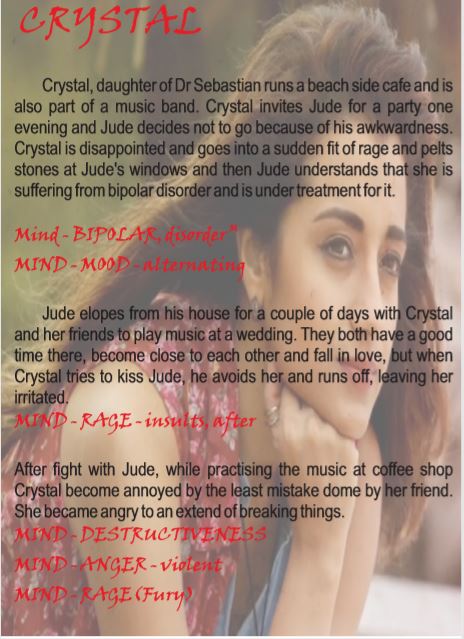
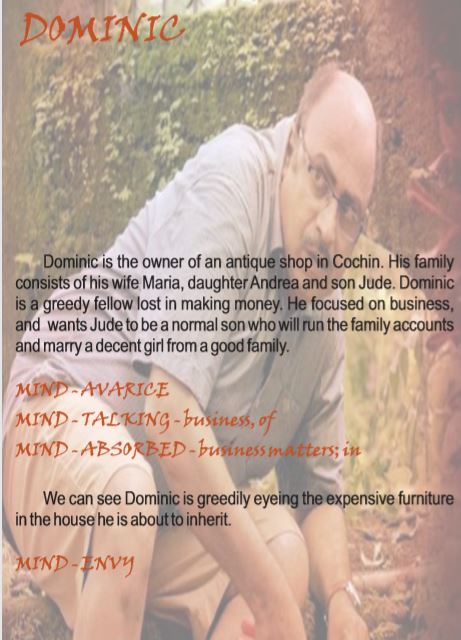
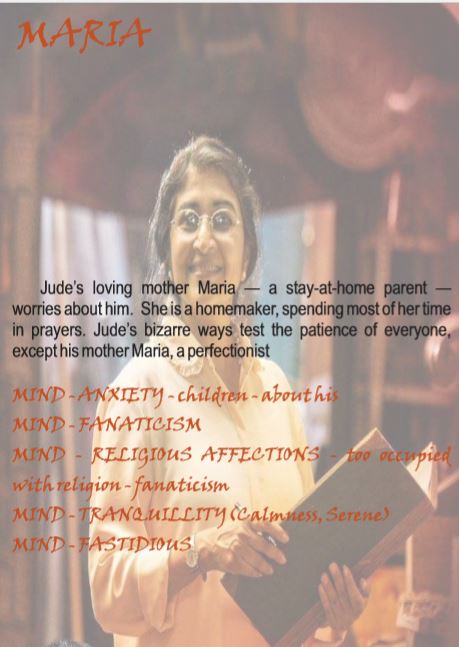
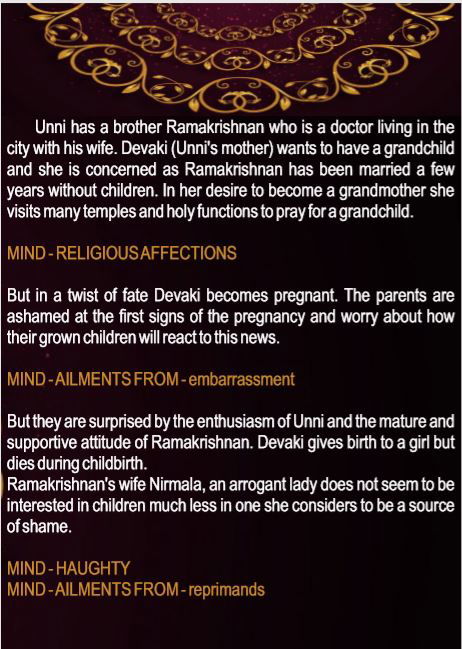
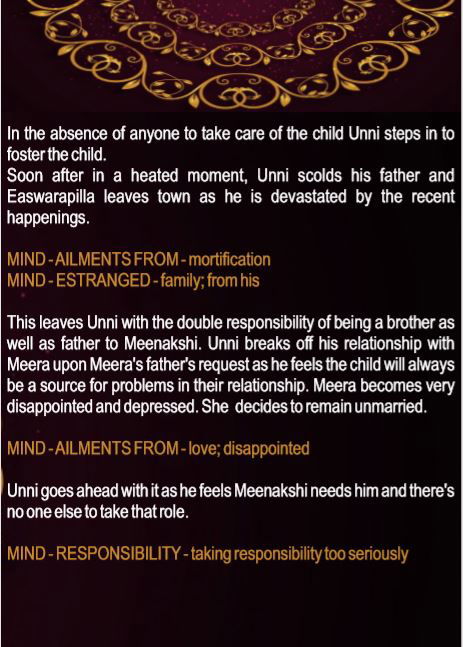
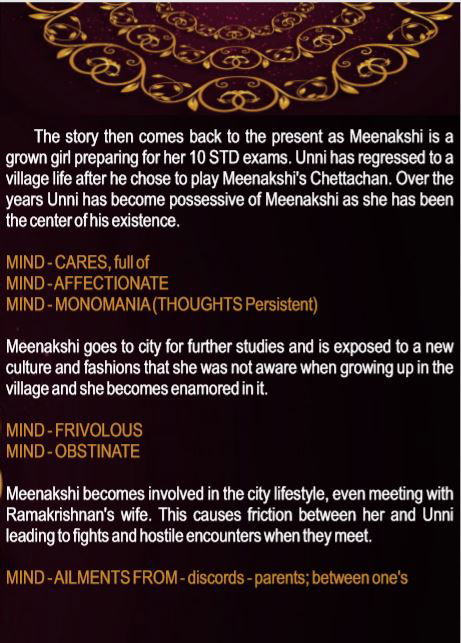
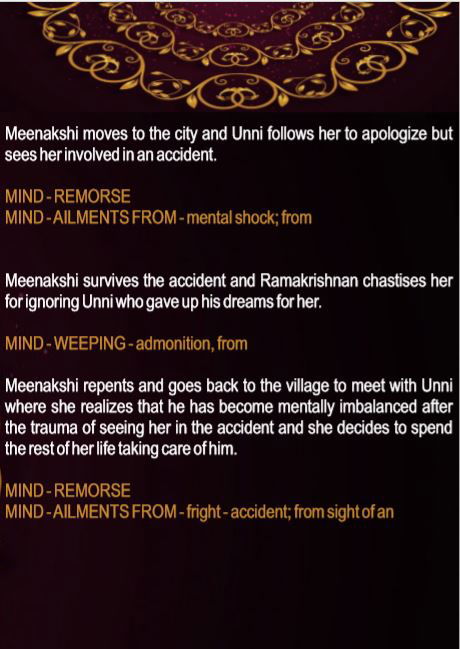
CASE SUMMARY
The facts in patient’s case are outlined in a narrative format to work out & they are an efficient way to excel in analysis & evaluation.
TERMINOLOGY- SYNTHESIS
Courtesy: www.homeobook.com
MIND
Acarophobia-Fear of insects
Acrophobia-Unusual fear of heights
Affability-friendly; courteous
Aichmophobia-Fear of pins
Ailurophobia-Fear of cats
Algophobia-fear of pain
Amathophobia-Fear of dirt
Amaxophobia-Fear of riding
Anarchist-a person who rebels against any authority
Anemophobia-Fear of wind/air
Animus –hostility; ill feeling
Anthropophobia-Abnormal fear of people or society
Aplomb-self assurance
Ardent-eager ; passionate
Ascetic –severely abstinent / self –denying (increased self control)
Astraphobia –morbid fear of thunder storms
Audacity-daring/bold
Autophobia-fear of being alone
Avarice-greed for wealth
Basphobia-fear of walking
Bellowing-deep loud roar
Belonephobia-Fear of pins
Benevolence-kind and helpful; charitable
Bereavement-deprive of friend or relative esp by death
Blasphemy-talk irreverently about
Brontophobia-fear of thunder storm
Calumniate-slander/ malicious misrepresentation
Catoptrophobia-Fear of mirrors
Chagrin-acute vexation/ disappointment.
Charlatan-falsely claiming knowledge or skill
Circumspection- Cautious/ taking everything into account
Clairaudient- The ability to hear sounds and voices that are outside of the natural range of hearing.
Condescending attitude-graciously consent to do a thing while showing one’s superiority/to be on equal terms with
Conformism-conventional; person who confirms to conventional practice
Contemptuous-showing contempt ( feeling that a person deserves reproach)
Contentious-quarrelsome
Coquettish-flirt
Culpability-deserving blame
Cynical-person with pessimistic view of human nature
Cynophobia-fear of dogs
Debauchery-excessive sensual indulgence
Defiant-open disobedience; bold resistance
Depreciation-decline in value
Desolate-uninhabited
Despotic-absolute ruler; tyrant
Discernment-having good judgement or insight
Dotage-feeble minded senility
Dromomania-pathologically strong desire to travel
Encopresis-involuntary passage of faeces
Ergasiaphobia-fear of responsibility/work
Exasperated-irritate intensely
Exultant-rejoice
Fanaticism-bsessively devoted to a belief
Fervent-intense/ ardent
Foppish-man excessively devoted to style and fashion
Frivolous-not serious/ silly
Gluttony-excessive eater/ insatiably eager person
Haphephobia-Fear of being touched
Imperious-over bearing; domineering
Impertinence-irrelevant;insolentImpetuous-acting rashly/ suddenly
Importunate-making persistent requests
Improvident-lacking foresight; wasteful
Imprudence-rash; indiscreet
Impudent-impertinent(irrelevant)Inexorable-relentless [relent-yield to compassion]
Intriguer-one who does underhand plotting; secret arrangement
Laconic-using few words
Lecherous-lustful
Litigious-contentious[ quarrelsome]
Lypothymia-a condition or feeling of faintness
Mendacity-lying; untruthful
Mysophobia-pathological fear of contamination or germs
Obsequious-exhibiting servile compliance; obedient in a servile manner
Obtunded-dull; less than full mental capacity
Pavor nocturnes-night terrors esp seen in children
Pedant-person who insists on strict adherence to formal rules
Perfidious-breach of faith
Pertinacity-persistent; obstinate
Petulant-impatient/ irritable
Ponophobia –fear of fatigue esp through over work
Presumptuous-unduly confident; arrogant
Reticent-avoidance of saying all one knows or feels; taciturnity
Reveling-make merry
Scorned-contempt; reject or refuse to do as worthy
Servile-like slave; subservient
Taciturn-uncommunicative
Taphephobia-fear of being buried alive
Temerity-rashness; audacity
Tipsy-slightly drunk; showing intoxication
Unscrupulous-unprincipled
Usurer-person who lends money at exorbitant or illegal rate
Vacillation-fluctuate in opinion/ resolution
Vagabond-wanderer; having no home
Vanity-unreal thing; conceit about one’s attainment or appearance
Wily-cunning
Xenophobia-unreasonable fear or hatred of foreigners or strangers
MIND
Acarophobia-Fear of insects
Acrophobia-Unusual fear of heights
Affability-friendly; courteous
Aichmophobia-Fear of pins
Ailurophobia-Fear of cats
Algophobia-fear of pain
Amathophobia-Fear of dirt
Amaxophobia-Fear of riding
Anarchist-a person who rebels against any authority
Anemophobia-Fear of wind/air
Animus –hostility; ill feeling
Anthropophobia-Abnormal fear of people or society
Aplomb-self assurance
Ardent-eager ; passionate
Ascetic –severely abstinent / self –denying (increased self control)
Astraphobia –morbid fear of thunder storms
Audacity-daring/bold
Autophobia-fear of being alone
Avarice-greed for wealth
Basphobia-fear of walking
Bellowing-deep loud roar
Belonephobia-Fear of pins
Benevolence-kind and helpful; charitable
Bereavement-deprive of friend or relative esp by death
Blasphemy-talk irreverently about
Brontophobia-fear of thunder storm
Calumniate-slander/ malicious misrepresentation
Catoptrophobia-Fear of mirrors
Chagrin-acute vexation/ disappointment.
Charlatan-falsely claiming knowledge or skill
Circumspection- Cautious/ taking everything into account
Clairaudient- The ability to hear sounds and voices that are outside of the natural range of hearing.
Condescending attitude-graciously consent to do a thing while showing one’s superiority/to be on equal terms with
Conformism-conventional; person who confirms to conventional practice
Contemptuous-showing contempt ( feeling that a person deserves reproach)
Contentious-quarrelsome
Coquettish-flirt
Culpability-deserving blame
Cynical-person with pessimistic view of human nature
Cynophobia-fear of dogs
Debauchery-excessive sensual indulgence
Defiant-open disobedience; bold resistance
Depreciation-decline in value
Desolate-uninhabited
Despotic-absolute ruler; tyrant
Discernment-having good judgement or insight
Dotage-feeble minded senility
Dromomania-pathologically strong desire to travel
Encopresis-involuntary passage of faeces
Ergasiaphobia-fear of responsibility/work
Exasperated-irritate intensely
Exultant-rejoice
Fanaticism-bsessively devoted to a belief
Fervent-intense/ ardent
Foppish-man excessively devoted to style and fashion
Frivolous-not serious/ silly
Gluttony-excessive eater/ insatiably eager person
Haphephobia-Fear of being touched
Imperious-over bearing; domineering
Impertinence-irrelevant;insolentImpetuous-acting rashly/ suddenly
Importunate-making persistent requests
Improvident-lacking foresight; wasteful
Imprudence-rash; indiscreet
Impudent-impertinent(irrelevant)Inexorable-relentless [relent-yield to compassion]
Intriguer-one who does underhand plotting; secret arrangement
Laconic-using few words
Lecherous-lustful
Litigious-contentious[ quarrelsome]
Lypothymia-a condition or feeling of faintness
Mendacity-lying; untruthful
Mysophobia-pathological fear of contamination or germs
Obsequious-exhibiting servile compliance; obedient in a servile manner
Obtunded-dull; less than full mental capacity
Pavor nocturnes-night terrors esp seen in children
Pedant-person who insists on strict adherence to formal rules
Perfidious-breach of faith
Pertinacity-persistent; obstinate
Petulant-impatient/ irritable
Ponophobia –fear of fatigue esp through over work
Presumptuous-unduly confident; arrogant
Reticent-avoidance of saying all one knows or feels; taciturnity
Reveling-make merry
Scorned-contempt; reject or refuse to do as worthy
Servile-like slave; subservient
Taciturn-uncommunicative
Taphephobia-fear of being buried alive
Temerity-rashness; audacity
Tipsy-slightly drunk; showing intoxication
Unscrupulous-unprincipled
Usurer-person who lends money at exorbitant or illegal rate
Vacillation-fluctuate in opinion/ resolution
Vagabond-wanderer; having no home
Vanity-unreal thing; conceit about one’s attainment or appearance
Wily-cunning
Xenophobia-unreasonable fear or hatred of foreigners or strangers
TRIBUTE TO OUR MASTER AND ALL REPERTORIANS
"likes are cured by likes”
SIMILIA SIMILIBUS CURANTER
CONTACT US
- Shree Vidyadhiraja Homoeopathic Medical College, Nemom, Thiruvananthapuram, Kerala - 695020



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}